病院概要
医療サービス
症状&治療
予約
料金表
インフォメーション
医師検索
保険&キャッシュレスサービス
設備
プロモーション
健康指針
ニュース&セミナー
当院連絡先
採用情報
2
日本語
EN
繁體
简体
日本語
EN
繁體
简体
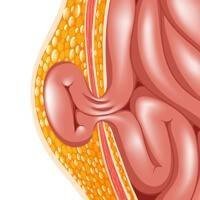
Hernia
Hernia is one of the most
common surgical problems
, affecting millions of people worldwide.
Please choose your hernia
Groin Hernia Suspected
I suspect you are having groin hernia, let's start our groin hernia assessment please.
Start Groin Assessment
Indirect Inguinal Hernia
Direct Inguinal Hernia
Femoral Hernia
Ventral Hernia Suspected
I suspect you are having ventral hernia, let us give you more information on ventral hernia.
Learn More
Umbilical Hernia
Epigastric Hernia
Incisional Hernia
Spigelian Hernia
戻る
関連医療業務
General Surgery & Minimally Invasive Surgery
Hernia Clinic
関連医師
General Surgery
Dr. Yang George Pei Cheung
Adventist Health Physician
Consultant In General Surgery
Clinical Director Of Robotic Surgery (General Surgery)
Profile
Timetable
予約
MBBS (UNSW, Aust)
MRCSEd
FRACS
FCSHK
FHKAM (Surgery)
General Surgery
Dr. Kwan Tim Lok
Adventist Health Physician
Consultant In General Surgery
Profile
Timetable
予約
MBBS (HK)
FRCSEd
FCSHK
FRCSEd (Gen)
FHKAM (Surgery)
関連文献
Hernia
Dr. Yang George Pei Cheung
2022年3月24日
Herniated Disk
Dr. Leung Clarence Hin Shuen
2022年8月4日
Inguinal Hernia
Dr. Yang George Pei Cheung
2022年1月1日
Related Brochures
Hernia Knowledge
医師
予約
WhatsApp Booking
Contact
トップ
警戒レベル
Hospital Services During Bad Weather
閉じる
閉じる
Outpatient clinic (GPs)
Office Hour: Sunday - Friday (9am - 1pm & 2pm - 6pm)
Waiting Time
予約